|
Abstract:
Background:
40%-60% of the patients with Obsessive-Compulsive Disorder (OCD) remain unimproved by Serotonin-Reuptake inhibitors. The objective of this study was to examine whether addition of olanzapine to Fluvoxamine is useful for patients with OCD who do not respond to SRI monotherapy.
Method:
Eleven patients with OCD (DSM IV-TR criteria) who had not responded to Fluvoxamine at maximum dose and duration were assigned to receive olanzapine in addition to their SRI for 12 weeks. Treatment response was assessed using the Yale-Brown Obsessive Compulsive Scale (YBOCS).
Results:
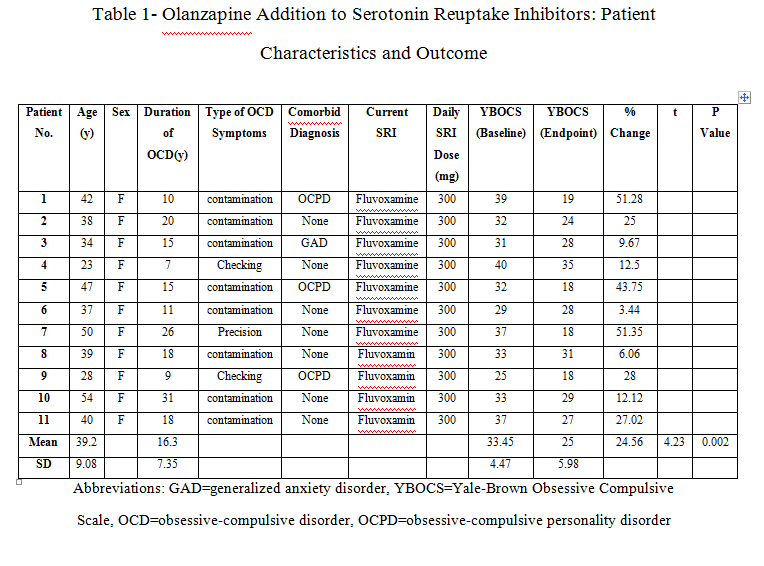
six of 11 patients respond to the olanzapine addition. The mean+/-SD baseline YBOCS score of 33.45 +/- 4.47 dropped to a mean of 25 +/- 5.98 at endpoint with a mean reduction of 24.56%.
Conclusion:
This study shows that treatment-refractory OCD Patients may benefit from addition of olanzapine to ongoing SRI therapy.
Key words:
Obsessive-compulsive disorder; treatment refractory; Olanzapine.
Introduction:
Serotonin Reuptake Inhibitors (SRIs) are the most effectual drug treatment accessible for obsessive-compulsive disorder (OCD). [1] Clomipramine, citalopram, fluoxetine, fluvoxamine, paroxetine, and sertraline have been proved to be effective against obsessive and compulsive symptoms independent of their antidepressant activity. [2, 3, 4] 50%-60% of patients with OCD fail to respond to a single trial of an SRI, and 20-40% does not respond sufficiently after several medication trials. [1] Moreover, although the selective serotonin reuptake inhibitors (SSRIs) are generally considered to be secure and well tolerated, still a proportion of subjects does experience intolerable side effects and discontinue treatment prematurely. Also, No single drug acting on different neurotransmitter systems has yet proved an absolute efficacy against obsessive-compulsive symptoms. Therapeutic strategies in these resistant cases usually consist of augmentation therapies with, tryptophan, buspirone, clonazepam and lithium or the addition of antipsychotic drugs. But the final results with these tactics were not en-couraging so far and have remained somewhat experimental than crucial. The addition of low-dose antipsychotics to standard antidepressant treatment has shown to be effective in some cases, but extrapyramidal side effects have limited the use of typical antipsychotics. Therefore treatment with atypical antipsychotic that shows fewer extrapyramidal symptoms might be a useful alternative for treatment-refractory OCD patients. Beneficial effects of adding risperidone to SSRIs have been observed in some cases of treatment-resistant obsessive compulsive disorder. [5, 6] In prior four open [7, 8, 9, 10] and one Double-blind [11] studies, there had been seen positive results with the addition of olanzapine to the regular antidepressant treatment of the patients.
Materials and Methods:
Universitys Medical Ethics Comity approved this study. Seven outpatients among clientele of two psychiatric clinics, and four inpatients from psychiatric wards of a psychiatric hospital, after full explanation of the procedure for them and obtaining signed informed consent, entered the study. All of the patients were female. The mean +/- SD age of the subjects was 39.2+/- 9.08 years. Patients were diagnosed as OCD according to the criteria of Diagnostic and Statistical Manual of mental disorders, 4th edition, text revision (DSMIV-TR). Inclusion criteria in this study were:
1. OCD symptoms resistant to Fluvoxamine at maximum dose and enough duration (12 weeks).
2. A score on the YBOCS [12] of at least 18.The subjects mean +/- SD baseline score on the YBOCS was33.45 +/- 4.47 and the mean duration of illness was 16.3+/-7.35 years. All of the patients had both obsessions and compulsions. In an open, 12-week trial, all patients continued to take their current SRI (Fluvoxamine) at the maximum dose (300mg/day) during addition. Olanzapine addition was initiated at a dose of 2.5 mg/day and then increased by 2.5 mg increments in weekly meetings, to a maximum of 10 mg by week4 and then this dose was held constant to the end of the study. No other psychotropic drug or psychosocial intervention (like Exposure Response Prevention) during the trial was administrated for them. Subjects were seen by the same trained rater at baseline and at the end of weeks 2, 4, 6, 8 and 12, at which times clinical response and adverse events were evaluated. The rater was not blind to treatment and its goals. The primary efficacy parameter was YBOCS score [12]. Full response to treatment was prospectively defined as at least 50% decrease in YBOCS score and partial response as at least 25% decrease in YBOCS score from beginning. Adverse events were assessed at each visit by means of patients' spontaneous reports and clinical examination by psychiatrist.
Results:
Two patients (one outpatient and one inpatient) were full responders with a mean decrease of 51% in YBOCS score. Four patients (three outpatients and one inpatient) were partial responders with at least a 25% decrease. Five patients (three outpatients and two inpatients) experienced no change in their obsessive-compulsive symptoms (Table 1). In those who benefited from the treatment, improvement started within the first two weeks of olanzapine addition. In general patients mean YBOCS score decreased significantly (by 24.56%) from baseline to endpoint (paired 2-tailed t test: t = 4.23, df = 10, p = 0.002).
The most common adverse effects of olanzapine in our samples were weight gain (n=2), somnolence (n=3), dizziness (n=2), dyspepsia (n=2), tremor (n=1), and constipation (n=1). Since the side effects were mild and well tolerated, no one dropped out owing to medication intolerance.
Discussion:
This study provides supplementary evidence that adding of olanzapine to ongoing SRI treatment may be efficacious for therapy-refractory OCD patients. There are, however, limitations to the data presented due to the small sample size and open-label design. In all, the results of our study are consistent with the findings of previous addition trials with risperidone and olanzapine. [5, 6, 7, 8, 9, 10, and 11] More patients (54%) in our trial had responded positively to the aforesaid augmentation, in comparison with Koran.LM (30%) [8] and Bogetto.F (43%) [9], although it was smaller than Weiss.El (70%) [7] and Francobandiera.G (60%) [10]. But may be this diversity is the outcome of dissimilarities between intervening factors, like the kind of prescribed SRI, duration of study, patient's gender, and the criteria of response. The main problem here is that there is some inconsistency in the definition of treatment refractoriness. Most studies included patients who had failed to respond to only one SRI trial. Also there is not yet any universal agreement on the definition of responsiveness or resistance in the realm of OCD in comparison with, for example, schizophrenia. For instance, Weiss et al. [7] used a cutoff of 50% decrease in YBOCS score as responders, while Francobanderia [10] chose a cutoff of 25%. On the other hand, McDougle et al [6] and Pallanti [11], preferred cutoff of 35% for YBOCS decrease and a final score of 16 on the YBOCS in combination with a final Clinical Global Impressions scale rating of much improved or very much improved. Partial response, also, is defined as 23-35% improvement in YBOCS score [11]. In this regard relapse was defined as a 25% worsening in YBOCS (or a CGI score of 6) after a period of remission and the term treatment-refractory has reserved for those who do not respond to all available treatments. [11] Such differences make difficult the comparison of effect sizes between studies. Unlike other studies, in this one, weight gain (18%) was not the most common side effect of olanzapine and dizziness and dyspepsia had the same prevalence too among our patients. Somnolence was the most prevalent side effect (27%). Additionally, all of them were mild to moderate and did not cause serious problem for the patients. Atypical antipsychotics may enhance the action of SRIs through serotonin receptor blockade. The broader range of effective treatment with the addition of atypical antipsychotics may be due to D2 blockade or a combined serotonergic-dopaminergic blockade, particularly a 5-HT2A and D2 antagonism. [5] Thus, addition of atypical antipsychotics to SRIs seems a promising pharmacotherapy intervention for treatment refractory OCD patients. Further investigations on the mechanism of action of these addition strategies for OCD are warranted. Small sample size, short duration of measurement, gender-based sampling, and open-label design were among the weak points of this study.
Conclusion: This study shows that treatment-refractory OCD Patients may benefit from addition of olanzapine to ongoing SRI therapy.
REFERENCES:
1. Fienberg NA, Bullock T, Montgomery DB, Montgomery SA. Serotonin reuptake inhibitors are the treatment of choice in obsessive-compulsive disorder. Clin Psychopharmacology. 1992; 7(suppl 1):43.
2. Mcdougle CJ, Gordman WK, Price LH. The pharmacotherapy of obsessive-compulsive disorder. Pharmopsychiatry.1993; 269(suppl):24 .
3. Hollander E, Kaplan A, Allen A, Cartwright C. Pharmacotherapy for obsessive-compulsive disorder. Psychiatric Clin North AM. 2000; 23(3):643.
4. Goodman WK, Price LH, Rasmussen SA, et al. Efficacy of fluvoxamine in obsessive-compulsive disorder: a comparison with placebo. Arch Gen Psychiatry 1989; 46: 36-44.
5. McDougle CJ, Fleischmann RL, Epperson CN, Et al. Risperidone addition in fluvoxamine-refractory obsessive-compulsive disorder: three cases. J Clin Psychiatry 1995; 56:526-528.
6. McDougle CJ,Epperson CN, Pelton GH,et al. A double-blind, placebo-controlled study of resperidone addition in serotonin reuptake inhibitor-refractory obsessive-compulsive disorder.Arch Gen Psychiatry 2000; 57: 794-801 .
7. Weiss El, Potenza MN, McDougle CJ , at el. Olanzapine addition in obsessive-compulsive disorder refractory to selective serotonin reuptake inhibitors; an open-label case series.J Clin Psychiatry 1999;60;524-527 .
8. Koran LM, Ringold AL, Elliot MA. Olanzapine augmentation for treatment-resistant obsessive-compulsive disorder. J Clin Psychiatry 2000; 61:514-517.
9. Bogetto F, Bellino S, Vaschetto P, et al. Olanzapine augmentation of fluvoxamine in refrectory obsessive-compulsive disorder (OCD): a 12-week open trial. Psychiatry Res 2000; 96:91-98.
10. Francobandiera G. Olanzapine augmentation of serotonin uptake inhibitors in obsessive-compulsive disorder: an open study.Can J Psychiatry 2001; 46:356-358.
11. Bystrisky A. Augmentation of SSRI response in refractory OCD using adjunct olanzapine: a placebo-controlled trial. In: New Research Abstracts of the 154th Annual Meeting of the American Psychiatric Association; May 9, 2001.
12. Goodman WK, Price LH, Rasmussen SA, et al. The Yale-Brown Obsessive Compulsive Scale, 1: development, use, and reliability. Arch Gen Psychiatry 1998; 46:1006-1011.
|